
According to wiktionary: The collapse of a part of or the whole lung caused by inner factors rather than a pneumothorax.
And, on Wikipedia.
And, on Wikipedia.
Another music post. Heard this band (Carousel Kings) on last.fm (link is to my profile), which supplies me with just the happy, poppy, easy sound I wanna hear when I am reading about doping geezers with rat poison. I think they deserve a listen if not only because they satisfy my 13 year old girl music taste.
If you are interested in pop punk and/or hip hop or just a cool sound, you might want to check out Secret Secret Dino Club. The band(? might be a one man operation, I'm not sure)'s work is a cool blend of two two genres for an interesting feel-good sound, just in time for summer. Also, they have steezy merch:




... but, now desperately need. Thanks, internet.
The top is blue, the bottom is green with Sebastian the Ibis. I don't know how exactly I would pull these off, but I do know that I would try. And at $165 they don't seem to be too bad a deal compared to the alternatives. I'd probably go Ibis-free, but had to rep. Also, they are a local (South Florida) company. Here is more info than you wanted to know about this genre of footwear. The genesis for this whole post is here.
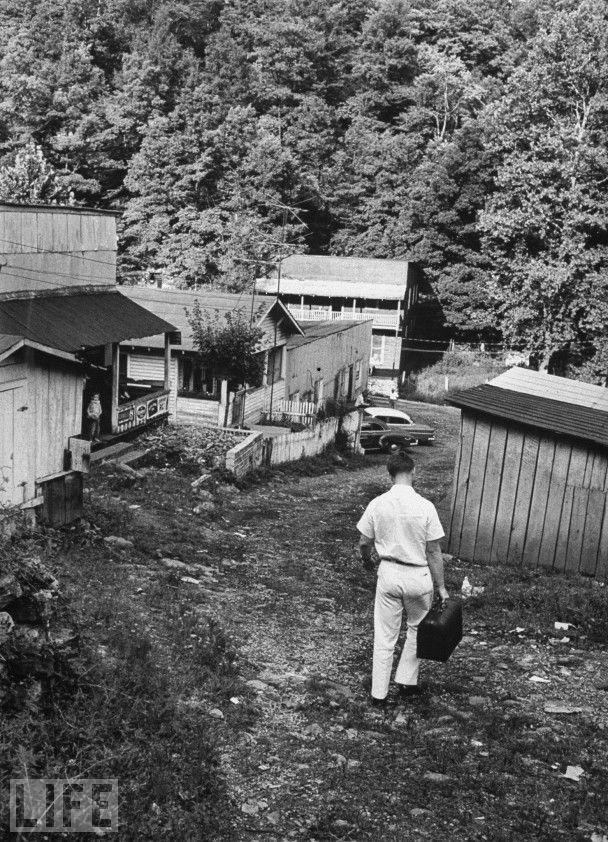



Doctor bags and the down home country docs who carry them have all but fallen completely off. The style and demeanor these gentleman display should serve as inspiration for current and future doctors. All of the photos are courtesy of the LIFE archive. And check out this EDC (holler).

... this. Simply put, it takes your Facebook Phonebook and downloads that to your Google Contacts which are then automatically synced with your phone's contacts.
edit: I had spelled Android 'Androis.' Androis is the French knockoff of Android.
edit: I had spelled Android 'Androis.' Androis is the French knockoff of Android.
... while watching some archival footage of med school lectures. The doctor giving the presentation said, "...should be 1-1.2 centimeters [pronounced saun-timeters ('saun' like 'sauna'] thick, whereas this is probably 2.5 centimeters [cent-imeters ('cent' like 'penny')]..." Dude needs to make up his mind.
This is a public service announcement to my fellow medical students in their basic science years. If your medical school is kind enough to use your tuition money to video record your lectures and post them on the internet for your later perusal, you do not -- I repeat -- do not need to buy any fancy software to speed up your lectures without chipmunking. Your free alternative to the expensive software, such as 2xAV by Enounce, is VLC media player. Just make sure that you have "Scale audio tempo in sync with playback rate" checked. You access this check box through the "Show setting -- All" radio button and then the "Filters" tab under "Audio."
Quick and dirty screenshot of the dialog:

Quick and dirty screenshot of the dialog:


Instead of studying, I just read this post at The Volokh Conspiracy on how the new-fangled health-care mandate is unconstitutional. There is a lot of (what I perceive to be) technical legal ideas in it (that I don't understand completely), but the logic interests me.
The really short version of the post is that the Supreme Court would not be looking at the constitutionality of the mandate in terms of how the drafters of the Constitution conceived of the government's powers. Instead, the Court will evaluate constitutionality of the mandate based on either: 1) if the mandate is consistent with what the Supreme Court has ruled before, or 2) public opinion of the mandate and personal political ideology (preference for the size and power of government).
"And this [option 2) above] would seem to be the epitome of the Rule of Men, as opposed to the Rule of Law."
The really short version of the post is that the Supreme Court would not be looking at the constitutionality of the mandate in terms of how the drafters of the Constitution conceived of the government's powers. Instead, the Court will evaluate constitutionality of the mandate based on either: 1) if the mandate is consistent with what the Supreme Court has ruled before, or 2) public opinion of the mandate and personal political ideology (preference for the size and power of government).
"And this [option 2) above] would seem to be the epitome of the Rule of Men, as opposed to the Rule of Law."
"Consider a porterhouse steak with a quarter-inch layer of fat. After broiling, this steak will reduce to almost equal parts fat and protein. Fifty-one percent of the fat is monounsaturated, of which 90 percent is oleic acid. Saturated fat constitutes 45 percent of the total fat, but a third of that is stearic acid, which will increase HDL cholesterol while having no effect on LDL... The remaining 4 percent of the fat is polyunsaturated, which lowers LDL cholesterol but has no meaningful effect on HDL. In sum, perhaps as much as 70 percent of the fat content of a porterhouse steak will improve the relative levels of LDL and HDL cholesterol, compared with what they would be if carbohydrates such as bread, potatoes, or pasta were consumed. The remaining 30 percent will raise LDL cholesteropl but will also raise HDL cholesterol and will have an insignificant effect, if any, on the ratio of total cholesterol to HDL. All of this suggests that easting a porterhouse steak in lieu of bread or potatoes would actually reduce heart-disease risk, although virtually no nutritional authority will say so publicly. The same is true for lard and bacon."
This speaks for itself.
This speaks for itself.
'Common good' is quite not the same as 'collective good.' If anyone tries to assert that a health insurance mandate or any other material thing is for the common good, politely inform them that what they mean is for the collective good. Common goods are good for everyone involved. Collective goods are good only for those who receive them as private goods. Here is a nice little article that sheds more light on the distinction.
Update
In February, around the time of this blog's inception, I posted about how I would try my damnedest to adhere to some new standards for myself. I said I would use the 6 Changes platform to break some old habits and create some new ones.
My experience so far is it is harder to break new habits than to ingrain new ones. That said, I haven't given up the onychophagia (technical for 'nail biting'), but I have been sticking to a fitness regimen (which includes exercise, dietary alteration, and should also begin to include meditation).
News
Lately, in my spare time, I have been poring over lots of research papers, blog and print media archives, all in the hopes of elucidating some calm water amidst the frantic seas of the dietetic sphere.
What I have learned so far is that I have a lot to learn if diet is going to inform my future practice of medicine (as rightly it should). So many doctors, it seems, have such a poor grasp of how diet influences the physiology and pathology of humans.
Up to now, I've found Dr. Harris at PaNu to have the simplest and most thorough commentary on what is right (few things) and wrong (most things) with current dietary advice. I recommend his blog for a read for a fresh perspective, even if you drink the current dietetic establishment kool-aid (lowercase 'k' and 'a').
My gut (pun intended) feeling, my chemistry background (I was a chemistry major undergrad), and some first-year medical schooling all tell me that following a program like PaNu is where it's at for ease-of-use and nutritional soundness.
As of yesterday, I received my crisp, new copy of Gary Taubes' Good Calories, Bad Calories, which is the precipitating work of Dr. Harris' content at PaNu and a veritable bible for lots of the rest of the "paleo" blogosphere. I may post my impressions of this very influential books as I get further into it, but in the meantime, I say you pick up a copy for yourself. Just reading through the prologue has me convinced that Taubes' writing style is well-informed, while staying crystal clear and entertaining (clarity and interest are sometimes left out of non-fiction like this).
In February, around the time of this blog's inception, I posted about how I would try my damnedest to adhere to some new standards for myself. I said I would use the 6 Changes platform to break some old habits and create some new ones.
My experience so far is it is harder to break new habits than to ingrain new ones. That said, I haven't given up the onychophagia (technical for 'nail biting'), but I have been sticking to a fitness regimen (which includes exercise, dietary alteration, and should also begin to include meditation).
News
Lately, in my spare time, I have been poring over lots of research papers, blog and print media archives, all in the hopes of elucidating some calm water amidst the frantic seas of the dietetic sphere.
What I have learned so far is that I have a lot to learn if diet is going to inform my future practice of medicine (as rightly it should). So many doctors, it seems, have such a poor grasp of how diet influences the physiology and pathology of humans.
Up to now, I've found Dr. Harris at PaNu to have the simplest and most thorough commentary on what is right (few things) and wrong (most things) with current dietary advice. I recommend his blog for a read for a fresh perspective, even if you drink the current dietetic establishment kool-aid (lowercase 'k' and 'a').
My gut (pun intended) feeling, my chemistry background (I was a chemistry major undergrad), and some first-year medical schooling all tell me that following a program like PaNu is where it's at for ease-of-use and nutritional soundness.
As of yesterday, I received my crisp, new copy of Gary Taubes' Good Calories, Bad Calories, which is the precipitating work of Dr. Harris' content at PaNu and a veritable bible for lots of the rest of the "paleo" blogosphere. I may post my impressions of this very influential books as I get further into it, but in the meantime, I say you pick up a copy for yourself. Just reading through the prologue has me convinced that Taubes' writing style is well-informed, while staying crystal clear and entertaining (clarity and interest are sometimes left out of non-fiction like this).
The Lew Rockwell Blog featured this article from Slate. I like it because it is both a good argument for tempering government public health and nutrition recommendations, the low-fat likes of which seem to go hand in hand with federal subsidies in food production (e.g., huge subsidies for anything corn, the single most destructive component of American processed food) and for the fact that saturated fat, when it constitutes a larger proportion of the diet, seems to be heart healthy, unlike processed carbohydrates.
This profound post, the content of which was written in 1994, at Lew Rockwell Blog has it exactly right. If you see a trend in my posts (linking out to '90s references), it's because we were a smarter country, world and species in the 90s (and not just because of genius masterpieces like this).
Clay Shirky on Cognitive Surplus
Here is a really nice video keynote address on a cool idea called Cognitive Surplus. Check it out and learn about some pop-psych/sociology. This idea really makes the Internet the game changer that it has become. I found this through Seth's Blog.
Here is a really nice video keynote address on a cool idea called Cognitive Surplus. Check it out and learn about some pop-psych/sociology. This idea really makes the Internet the game changer that it has become. I found this through Seth's Blog.
Our Healthcare "System"
For ya'll that don't follow healthcare or don't quite understand how it works in this country, our healthcare system is actually a smorgasbord of systems rolled into one cluster-youknowwhat. According to a healthcare lecture I attended, the US has: private insurance (mostly) through employers (aka Socialized Health Insurance like in Germany); the state health system like the UK (care to the military, the VA system and to Native Americans); national health insurance similar to the Canadian system (Medicare for the aged and Medicaid for the poor, disabled or lucky) and out-of-pocket financing like the system they have in Cambodia and other non-developed nations (for young, working folks who don't think they need insurance or can't afford it).
Two headlines from my "AMA Morning Rounds" e-mail
'Fewer doctors accepting new Medicaid patients.'
If we move to a system where everyone is compulsorily "insured," and where everyone has equal coverage (does redistribution of wealth/resources ever work out fairly?), and where the fruits of one man's labor becomes another man's 'right,' doctors might even stop accepting patients who are have so-called private (but highly government-regulated) "insurance." When wages don't justify the work, doctors will eitheproviding services quit or demand payment for services in cash.
'North Carolina to issue preferred drug list for Medicaid patients.'
This headline is an example of a concept called care-rationing, whereby a finite medical resource is divvied by the government. Bureaucrats, not physicians, decide who may have what treatment and when.
For a good primer on some first principles related to government intervention in health care check out this video of Leonard Peikoff giving his speech, "Health Care is Not a Right."
Peikoff gave this in late 1993 in response to the Clinton plan.
Unfortunately, there isn't enough talk like this going on in response to ObamaCare.
This should be recommended reading for the all the squabblers in DC arguing the fine points of two evils, may the lesser of which win.
A transcript is here.
Peikoff gave this in late 1993 in response to the Clinton plan.
Unfortunately, there isn't enough talk like this going on in response to ObamaCare.
This should be recommended reading for the all the squabblers in DC arguing the fine points of two evils, may the lesser of which win.
A transcript is here.
From this article:
The italics are the author's.
I like good analogies for medical issues. This is one such analogy.
Bottom line: Before we talk about adding more proverbial mouths to feed with proverbial food we don't have, let's talk about how we are going to change our country's health care priorities.
Estimating how much the nation will spend on health care is difficult, but in many ways, it is even more difficult to say how much the nation should spend on health care, because the answer depends on values as well as on data related to health, medical technology, and the economy. This is the conceptual problem related to health care spending. A useful way to think about this "should" question is to imagine a family with a limited income trying to decide how much to spend on food, clothing, entertainment, and other activities. In principle, the family will get the most satisfaction from its income if it allocates it among the various goods and services in such a way that the last dollar spent in each category brings the same amount of satisfaction. If the family cannot achieve such equality, the total satisfaction could be increased by switching some spending from categories in which the last dollar spent provided less satisfaction to those in which the last dollar spent provided more satisfaction.
The italics are the author's.
I like good analogies for medical issues. This is one such analogy.
Bottom line: Before we talk about adding more proverbial mouths to feed with proverbial food we don't have, let's talk about how we are going to change our country's health care priorities.
Or so a recent paper indicates.
Blog Neuroskeptic posts on a recent paper that features the case of a 20-something guy with a genetic deficiency of a certain enzyme that doesn't allow him to make a bunch of chemicals necessary for 'normal' brain function. One such of these chemicals is serotonin, whose action is controlled by many anti-depressants.
Since my med school class an I are studying some neuroscience and it psychiatric aspects, this finding is quite intriguing. I was not able to pull up the original article for which the post is based, but will when I go to school tomorrow and can (ab)use my academic primary source privileges.
Also, I haven't fully investigated the blog from whence this post comes, but I am adding it to my feed, if not only for the remainder of neuroscience class. Looks like a good read. And, I always appreciate a dose of skepticism.
Blog Neuroskeptic posts on a recent paper that features the case of a 20-something guy with a genetic deficiency of a certain enzyme that doesn't allow him to make a bunch of chemicals necessary for 'normal' brain function. One such of these chemicals is serotonin, whose action is controlled by many anti-depressants.
Since my med school class an I are studying some neuroscience and it psychiatric aspects, this finding is quite intriguing. I was not able to pull up the original article for which the post is based, but will when I go to school tomorrow and can (ab)use my academic primary source privileges.
Also, I haven't fully investigated the blog from whence this post comes, but I am adding it to my feed, if not only for the remainder of neuroscience class. Looks like a good read. And, I always appreciate a dose of skepticism.
The NEJM has an interesting editorial on using whole individual genomes to assess for risk factors of disease.
The editorial concisely introduces the function of genomics and mutation analysis in medicine. It also addresses the current limitations and the promising future of the technology in patient care.
If you are unfamiliar with the medical (and other scientific) literature, editorials such as this often accompany the presentation of original research. In this case, the original study was this paper on Charcot-Marie-Tooth disease.
As it was the inspiration for the editorial, the original paper shows how sequencing the genomes of a proband (the technical term for the patient or individual who presents with a heritable disorder like Charcot-Marie-Tooth) and members of his or her family who also have the disease can allow scientists to pinpoint the genetic slips which cause disease.
In the paper, the investigators "identified a family with a recessive form of Charcot–Marie–Tooth disease for which the genetic basis had not been identified" or in other words, they took a case of disease whose genetic cause, slightly jumbled or abnormal DNA sequences, had not been identified. They took parts of the proband's DNA that were likely to be implicated in the disorder from the entire sequenced genome and compared it to select pieces of genome from family members that also had disease symptoms.
This comparison between proband genetic code and family member genetic code allowed investigators to positively identify underlying genetic problem in this form of the disease.
This information can then be used for diagnosis and treatment planning of the condition in others. As more associations of diseases (and even heritable factors which predispose people to diseases) with distinct genetic slips are made and technology to sequence and identify these slips becomes cheaper and more widespread, this technology will become commonplace in the provision of healthcare. This has many exciting implications, as well as a few problematic ones. As the editorial asks,
Despite these serious concerns (which will doubtlessly be resolved as practitioners embrace the new methods), it is exciting to me to be learning the practice of medicine amidst scientific advances such as these.
One note: Channeling University Diaries, one of my favorite education-related blogs, I caught this error in word choice from the editorial discussed above: "The field has been driven by saltatory leaps in technology."
Saltatory (commonly used with the word 'conduction,' as in 'saltatory conduction,' to describe how an electrical signal travels in a certain type of nerves) means that the thing in question 'proceeds by leaps rather than by smooth, continuous variation." Therefore to call something a 'saltatory leap' is redundant. This is hardly a common mistake, but a mistake no less.
The editorial concisely introduces the function of genomics and mutation analysis in medicine. It also addresses the current limitations and the promising future of the technology in patient care.
If you are unfamiliar with the medical (and other scientific) literature, editorials such as this often accompany the presentation of original research. In this case, the original study was this paper on Charcot-Marie-Tooth disease.
As it was the inspiration for the editorial, the original paper shows how sequencing the genomes of a proband (the technical term for the patient or individual who presents with a heritable disorder like Charcot-Marie-Tooth) and members of his or her family who also have the disease can allow scientists to pinpoint the genetic slips which cause disease.
In the paper, the investigators "identified a family with a recessive form of Charcot–Marie–Tooth disease for which the genetic basis had not been identified" or in other words, they took a case of disease whose genetic cause, slightly jumbled or abnormal DNA sequences, had not been identified. They took parts of the proband's DNA that were likely to be implicated in the disorder from the entire sequenced genome and compared it to select pieces of genome from family members that also had disease symptoms.
This comparison between proband genetic code and family member genetic code allowed investigators to positively identify underlying genetic problem in this form of the disease.
This information can then be used for diagnosis and treatment planning of the condition in others. As more associations of diseases (and even heritable factors which predispose people to diseases) with distinct genetic slips are made and technology to sequence and identify these slips becomes cheaper and more widespread, this technology will become commonplace in the provision of healthcare. This has many exciting implications, as well as a few problematic ones. As the editorial asks,
Who will benefit from comprehensive sequencing? When in a person's life should sequencing be done? How should we deal with the many variants of uncertain clinical significance? How should we interpret changes found outside of genes? How should we effectively communicate the results to patients in ways that will improve health without inducing neurosis?
Despite these serious concerns (which will doubtlessly be resolved as practitioners embrace the new methods), it is exciting to me to be learning the practice of medicine amidst scientific advances such as these.
One note: Channeling University Diaries, one of my favorite education-related blogs, I caught this error in word choice from the editorial discussed above: "The field has been driven by saltatory leaps in technology."
Saltatory (commonly used with the word 'conduction,' as in 'saltatory conduction,' to describe how an electrical signal travels in a certain type of nerves) means that the thing in question 'proceeds by leaps rather than by smooth, continuous variation." Therefore to call something a 'saltatory leap' is redundant. This is hardly a common mistake, but a mistake no less.
I strive for consistency with this space and I am trying to post daily.
As such, some of my posts will be themeless or mediocre or both. Hopefully, they will amuse you at least a little bit.
Why I skipped class today
Today, I went quail hunting with my grandpa here in South Florida. Between the two of us, we bagged 26. Not bad, I'd say, for a newb and a hard-of-sight octogenarian.
Moms and HHGG Connection
Q: What are mothers for?
A: Sending you and your siblings links like this.
In case you don't want to click the link, it features weather.com public service infonouncement on what to do should your vehicle suffer tire blowout.
The best suggestion from the whole piece is: Do not panic.
I addend the piece with: Always know where your towel is.
As such, some of my posts will be themeless or mediocre or both. Hopefully, they will amuse you at least a little bit.
Why I skipped class today
Today, I went quail hunting with my grandpa here in South Florida. Between the two of us, we bagged 26. Not bad, I'd say, for a newb and a hard-of-sight octogenarian.
Moms and HHGG Connection
Q: What are mothers for?
A: Sending you and your siblings links like this.
In case you don't want to click the link, it features weather.com public service infonouncement on what to do should your vehicle suffer tire blowout.
The best suggestion from the whole piece is: Do not panic.
I addend the piece with: Always know where your towel is.

Does anyone else find this image funny?
This is a rather antiquated image from a lecture of mine on head injury.
On the original .ppt slide show, it looked like a digitalization of an old slide (you know, like when you had take a film picture of your diagram and have it made at a photo shop or whatever).
The intent of the graphic is, apparently, to illustrate the phenomena of herniation (brain pushing out of skull) and compartment syndrome (general term for compression of tissue inside closed spaces in the body).
All I see is a bulimic tomato.

Funny, irreverent cartoon by one of my classmates (He is also participating in the MWC 100 Days of Burpees Challenge.). Shows that med students can have a sense of humor sometimes, too. Originally posted here.

Jackson Hospital System is canning a bunch of employees and boarding-up two of its suburban facilities.
OPM stands for 'Other People's Money,' a term I picked up at a lecture by Eric Kriss, who was a big player in the 2006 healthcare reform in Massachusetts. Huge surprise that OPM eventually dries up. (10) Also, interesting to me that hardworking folks (we'll let the fact that a lot of them are union members slide) are gonna be out of a job because of a community's decision to make institutional healthcare a "right" for all comers, regardless of blah, blah, blah.
OPM stands for 'Other People's Money,' a term I picked up at a lecture by Eric Kriss, who was a big player in the 2006 healthcare reform in Massachusetts. Huge surprise that OPM eventually dries up. (10) Also, interesting to me that hardworking folks (we'll let the fact that a lot of them are union members slide) are gonna be out of a job because of a community's decision to make institutional healthcare a "right" for all comers, regardless of blah, blah, blah.
Late last month, I resolved that, starting March 2 (a day after a med school test cycle was completed), I would stop biting my nails. So far, I have failed. I know it is early, but this is going to be more difficult than I anticipated. Here are some observations I have made about my habit-breaking experience:
Trigger identification: Many habits, learned and unlearned, good and bad, are often accompanied by a set of triggers.
Triggers may be direct (smoking on the way to work in your car, at lunch break and after work lets out).
Some triggers may be more diffuse (nervous fidgeting, only be when you are stressed from work or school).
My issues: I have no idea when/why I bite my nails. I do it unconsciously. The only trigger I can reliably see is biting when I am in a dark room watching a movie, like at a class showing of a psychology movie. The biting is exacerbated by suspense, but I still bite in lighter movies with lighter subject matter.
Rationalization/Intellectualization: Even if an individual is conscious of their habit or become so while in the act, because of brain chemistry, that individual tends to make reasons for why the action is hunky-dory.
My issue: Once I begin biting a nail, I "have to" keep biting it to fix my own aberrant creation.
These are strong forces working against negative habit-changers. Warriors, stay strong. Onlookers, wish us luck.
Trigger identification: Many habits, learned and unlearned, good and bad, are often accompanied by a set of triggers.
Triggers may be direct (smoking on the way to work in your car, at lunch break and after work lets out).
Some triggers may be more diffuse (nervous fidgeting, only be when you are stressed from work or school).
My issues: I have no idea when/why I bite my nails. I do it unconsciously. The only trigger I can reliably see is biting when I am in a dark room watching a movie, like at a class showing of a psychology movie. The biting is exacerbated by suspense, but I still bite in lighter movies with lighter subject matter.
Rationalization/Intellectualization: Even if an individual is conscious of their habit or become so while in the act, because of brain chemistry, that individual tends to make reasons for why the action is hunky-dory.
My issue: Once I begin biting a nail, I "have to" keep biting it to fix my own aberrant creation.
These are strong forces working against negative habit-changers. Warriors, stay strong. Onlookers, wish us luck.
Since exercise is part of my new year's resolutions, I will start using this blog not just a platform for expression and my personal betterment, but also as a workout log (GPP stands for General Physical Preparedness). I may organize it later so that the log facet is a separate, less obtrusive feed, but for now, this is what we are working with.
Because it is simple, open-source (read free, with included school gym membership) and it gets results (like they say on the CF forums, "it's like it works"), I will be sticking to a 3 day on, 1 off regimen of CrossFit, if I can swing it and don't blow myself on WOD days 1 and 2.
For now, I'll be cherry picking the main page WODs. Today's workout for me was 100222.
As far as my logging goes, I will be trying over time to standardize my logging to make it search-able and easily tidy-able for analysis.
Because it is simple, open-source (read free, with included school gym membership) and it gets results (like they say on the CF forums, "it's like it works"), I will be sticking to a 3 day on, 1 off regimen of CrossFit, if I can swing it and don't blow myself on WOD days 1 and 2.
For now, I'll be cherry picking the main page WODs. Today's workout for me was 100222.
As far as my logging goes, I will be trying over time to standardize my logging to make it search-able and easily tidy-able for analysis.
Surfing the tubes and came upon this TED talk. I didn't read too much into how they calculate the risk numbers or what the risk really means, but I like the nice visual representations of data.
Check yours out here.
Check yours out here.
My classmates and I had our first neuroscience test this morning. My writing this post signifies that it is over and test study mode does not begin again until the second neuroscience test at the end of March.
That said, as I was catching up on my blog feed and other daily life things that I put off in favor of stressing and memorizing/promptly forgetting, I ran across this post in the ACP Internist, which is a re-blog of this post from Musings of a Distractible Mind, a blog by a (seemingly prolific) blogging primary care physician.
If you don't want to click the links, they feature an allegory for the current healthcare debate. It essentially raises the following question:
Why are the only choices we have a single-payer (gubmint) system and a (supposedly) free market (private) system?
Neither choice solves the real problem. The cost of our country's collective healthcare tab and the quality of the product it receives is incongruous. And, while I neither see doctors' paychecks not receive one myself (yet ), I am pretty sure that it is not the doctors' paychecks that are adding up to the umpteens of billions of dollars that go to healthcare in the country.
), I am pretty sure that it is not the doctors' paychecks that are adding up to the umpteens of billions of dollars that go to healthcare in the country.
What can we, as individuals, do about it? This is a topic for another post.
That said, as I was catching up on my blog feed and other daily life things that I put off in favor of stressing and memorizing/promptly forgetting, I ran across this post in the ACP Internist, which is a re-blog of this post from Musings of a Distractible Mind, a blog by a (seemingly prolific) blogging primary care physician.
If you don't want to click the links, they feature an allegory for the current healthcare debate. It essentially raises the following question:
Why are the only choices we have a single-payer (gubmint) system and a (supposedly) free market (private) system?
Neither choice solves the real problem. The cost of our country's collective healthcare tab and the quality of the product it receives is incongruous. And, while I neither see doctors' paychecks not receive one myself (yet
), I am pretty sure that it is not the doctors' paychecks that are adding up to the umpteens of billions of dollars that go to healthcare in the country.What can we, as individuals, do about it? This is a topic for another post.
 Figure 1: Inspired by a graph in this article, showing that the % of fatties in the US has increased while the % of energy consumed in fat has decreased, where there was no upward or downward trend before government recommendation and popular opinion was to decrease fat intake.
Figure 1: Inspired by a graph in this article, showing that the % of fatties in the US has increased while the % of energy consumed in fat has decreased, where there was no upward or downward trend before government recommendation and popular opinion was to decrease fat intake.As I was skimming the JAMA from a couple of weeks ago, I found this article that addresses the idea of government recommendations regarding diet and their impact on public "health." The gist is that (surprise, surprise) many government recommendations with respect to how to eat and exercise are not based on sound evidence and therefore are misguided and misleading for the public. The authors caution public health agencies to think twice about regulating salt content of prepared foods and lowering dietary sodium recommendations.
Then, I ADD-style pulled up one of the references in the paper because I saw it is about fat, my favorite food group (more to come soon about my nutritional habits). This paper is a critique of the dietary fat reduction recommendations by the USDA and USDHHS in the '80s that is based on bad or little evidence that lowering fat is beneficial or at the very least not harmful. It features the original version of Figure 1 above. Check it out yourself for an interesting read.
I posted yesterday about how I am going to concertedly make some life changes in the near future and concurrently be mindful of the how and why of the process.
In my post, I mentioned Zen Habits but did not mention that author's corollary project, 6 Changes. 6 Changes showcases a common-sense approach to changing/making/breaking habits.
The method includes identifying six (only six, no more, no less) habits to acquire or de-ingrain in a year's time, with a few steps to follow to acquire/un-acquire the habit.
As a professional student, I am staring down the barrel of my professional life. Since my professional life implies much physical contact and close interaction with near strangers, I am resolved to stop biting my fingernails, a nasty and unhygienic habit I have had for literally as long as I can remember.
This post serves as my 'very public' commitment (step 3; even though my readership is probably zero at this point). While I am already started on gaining the anti-habit, I officially start Tuesday morning.
Now that the cat is out of the bag, I will post my progress here intermittently. Thanks for the help, interwebz.
In my post, I mentioned Zen Habits but did not mention that author's corollary project, 6 Changes. 6 Changes showcases a common-sense approach to changing/making/breaking habits.
The method includes identifying six (only six, no more, no less) habits to acquire or de-ingrain in a year's time, with a few steps to follow to acquire/un-acquire the habit.
As a professional student, I am staring down the barrel of my professional life. Since my professional life implies much physical contact and close interaction with near strangers, I am resolved to stop biting my fingernails, a nasty and unhygienic habit I have had for literally as long as I can remember.
This post serves as my 'very public' commitment (step 3; even though my readership is probably zero at this point). While I am already started on gaining the anti-habit, I officially start Tuesday morning.
Now that the cat is out of the bag, I will post my progress here intermittently. Thanks for the help, interwebz.
Zen Habits has a post today about sticking to new habits here. This is quite relevant to my life as I am formulating a post right now about my late New Year's resolutions. I will use this blog as a tracking and public accountability platform. Also, this is my "Do it, no matter how badly" post for the day, as one of the habits I am trying to enforce in myself is writing more (to the tune of one post or creative piece a day), and better (let the interwebz be my judge). Some of the changes I am planning for my life or have already begun implementing include: diet, exercise, school, style and liesure. Look forward to reading more in the near future.
I am studying for a neuroscience test at the moment. Here is a dramatic YouTube example of physiologic nystagmus response to cold water stimulation of the horizontal ducts:
UBO - unidentified bright object, as in a periventricular white matter lesions in some cases. See here for an example, these from MS (so, not so unidentified).
I'm a first-year medical student at a private medical school in a large metro area. My general interests include: medicine, bike racing, general fitness, nutrition/food, and men's style.
I will use this blog to discuss my above interests and current events related to them. Hopefully, this will also give me a chance to improve my writing and improve my chances of reading more and more often, thereby making me a more well-rounded individual.
I will use this blog to discuss my above interests and current events related to them. Hopefully, this will also give me a chance to improve my writing and improve my chances of reading more and more often, thereby making me a more well-rounded individual.
Subscribe to:
Posts (Atom)